Osseointegration procedure
")
Our private Osseointegration procedure services are provided at the Royal Free Hospital, Hampstead.
To find out more about our hospitals click here:
Major limb osseointegration, is usually performed as a 1-stage operation. Historically, a 2-stage procedure was performed with a gap of 4 to 6 months between each stage. However, experience has confirmed that a single-stage procedure results in faster patient rehabilitation and minimises the risks (especially infection) associated with multiple procedures.
However, depending on the individual patient, multiple, staged procedures may still be required. This is particularly true when performing osseointegration surgery in the head and neck region or in the hand.
Surgery

Surgery to insert a bone-anchor differs depending on where the anchor is being placed. Surgery is usually performed under general anaesthesia. This will be augmented with a spinal or epidural block (for lower limb patients) or brachial plexus nerve block (for upper limb patients). In some cases, surgery may be performed under spinal or brachial plexus block alone, together with intravenous sedation.
To see details of the surgery to place a bone-anchor in the craniofacial skeleton, click here.
To see details of the surgery for hand osseointegration, click here.
When placing a bone-anchor into the upper or lower limb, an incision is made at the distal end of the stump. The tissues are then opened up in layers to expose the end of your residual bone. Using special instruments, the end of the bone is prepared by removing any unwanted soft-tissue, bony spurs or areas of heterotopic ossification (heterotopic ossification is the term given to the presence of bone in the soft tissues where bone does not normally exist). Your surgeon will then explore and deal with any neuromas – using the techniques described on our other webpages.
The residual muscles will be re-organised and grouped in a circumferential manner by attaching them directly to the bone. This will allow you to have better control over the residual limb in the future and also helps to create and maintain a stable, soft-tissue/implant interface.
The bone canal is now prepared by sequential reaming using special instruments that convert the bony canal from an oval to a cylindrical shape. Broaches that match the shape of the implant are used to create the final shape of the bony canal. Any bone that is removed during this process is carefully saved for potential use as a bone-graft. The implant cavity is now ready, and the implant is carefully pushed into the bony canal that has been prepared. If needed, the bone-graft can now be inserted to augment the fit.
To close the end of the stump, a skin flap is now prepared by removing some of the excess subcutaneous fat. This skin flap is then used to cover the muscles and the implant and is secured in place using surgical sutures and stainless stell staples. A circular opening (stoma) is created in the skin flap through which the tip of the implant can project through the skin.
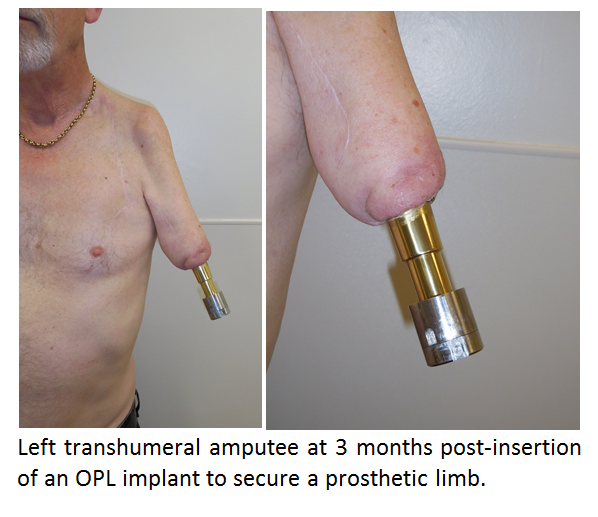
A dualcone is now attached to the end of the bone-anchor. All the connector components for your prosthesis will (eventually) be attached to the dualcone. These connector components are supplied by our rehabilitation partners (Dorset Orthopaedics) and will be fitted after your discharge from the Royal Free Hospital.
For more details on the rehabilitation process after insertion of a bone-anchor, click here.
Osseointegration